
DIAGNOSIS
New Born Screening
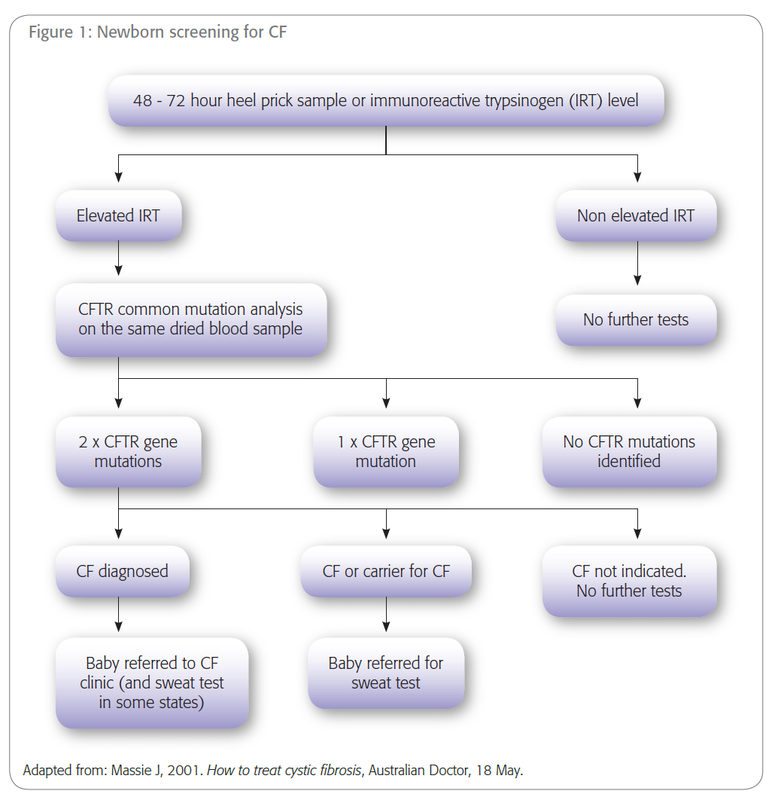
Newborn screening will detect the majority (95%) of babies with CF. Newborn screening is performed on all babies 48 to 72 hours after birth. Immunoreactive trypsinogen (IRT) is measured in a dried bloodspot from a heel-prick test (Guthrie test, newborn screening card). Raised IRT is an indication for DNA testing for CFTR mutations, which is also performed on the heel-prick sample. Each State and Australia screens for a different number of mutations depending on the frequency of the mutations in those States. The presence of two CFTR gene mutations is diagnostic of CF. A repeat blood sample may be collected to confirm the diagnosis and a sweat test may also be performed. If one CFTR gene mutation is present, the baby is considered at increased risk and a sweat test is performed. Eleven babies out of every 12 requiring a sweat test, on the basis of newborn screening results, do not have CF, but are simply carriers (have one mutation, ie hetero zygote). If no CFTR gene mutations
are detected, the baby is considered to be at low risk of having CF and no further
testing is performed. Babies with CF caused by mutations other than those
tested in the screening program(s) will be in this group and will therefore be
missed by newborn screening. The Newborn Screening Program-me in each
State/Territory coordinates or recommends referral for sweat testing and
genetic counseling. If a sweat test is required, the GP or pediatrician will
be contacted if their details are on the newborn screening card or held by the
hospital that delivered the baby. GP's then have the option of informing the family
themselves or asking the genetic counselor to do so. Feedback from families
suggests they prefer to be contacted with results by someone known to them.
CF may be missed by newborn screening for one of the following reasons:
CF may be missed by newborn screening for one of the following reasons:
- Screening sample not collected
- IRT is not raised
- Condition caused by mutations other than those tested in screening
- The sweat test is negative
Sweat test
Sweat tests measure chloride and sodium levels in sweat. They can be performed at any time from 1 week of age, but adequate sweat volumes may not be obtained before 6 weeks of age. Sweat test results are usually available within 24 hours and often on the same day. If there is clinical suspicion of CF, a sweat test should be arranged, even if the patient has had newborn screening, since approximately 5% of CF cases are not detected by newborn screening. Occasionally, sweat test results will be equivocal and a repeat will be required. Sweat tests can be difficult to perform and interpret, and should only be performed by an experienced clinician and laboratory staff. Sweat electrolyte values in adults are often higher than children and need to be interpreted by an expert. Patients who live in the country may need to travel to a CF center for a sweat test.
DNA Test
DNA testing for CF is performed during newborn screening or as a result of a positive sweat test or clinical suspicion. Genetic testing may be considered as a starting point for diagnosis if access to sweat testing is difficult. Discussion of such cases with a CF physician may be helpful. When a couple have had a baby with CF it is helpful to know the CFTR gene mutations to facilitate genetic counselling for subsequent pregnancies and accurate carrier testing for family members (cascade testing). Contact Genetics Services to find out which CFTR mutations are commonly tested for in your State or Territory (See Contacts, support and testing). Knowledge of ancestry can assist the detection of gene mutations. CF mutation screening can diagnose at least 80% of people with CF. Sweat testing is more definitive. Carrier testing can be offered to couples who have no family history, currently on a user-pays basis
